
1. Know what happened to your accessory nerve
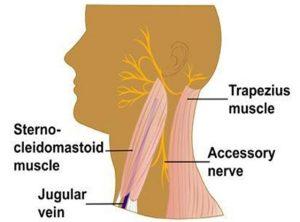
As I mentioned previously, there is an enormous amount of variability with respect to how much the accessory nerve will recover over time, if at all. The most important variable to consider, is what happened to your accessory nerve during your surgery.
During your surgical follow up, ask your surgeon what happened to your accessory nerve during surgery: was it cut, cut and sewn back together, stretched/retracted (most common), or untouched (unlikely)? This is critical in being able to predict how much you can expect the nerve (and thus your shoulder function) to recover.
2. Start with shoulder shrugs
Assuming your nerve was not removed or cut, shoulder shrugs can be a great place to start your recovery. Use the trapezius muscle to raise the shoulders up and down. Even if you cannot physically do the exercise, getting yourself into the position and visualizing yourself doing it can help begin to restore the connection between the nerve and the muscle. Be consistent with this exercise and be patient; it can take months for the nerve and the muscle to restore their “communication.” Want to learn how to do this exercise? I have created a video of this exercise to help you out.

3. See an experienced cancer rehab physiotherapist
Ultimately, the shoulder girdle is complex. Seeing a cancer rehab physiotherapist can be a really useful way to get help progressing beyond this simple shoulder shrug exercise into more complex and functional movement patterns.
(April is National Oral, Head & Neck Cancer Awareness Month. Please share this blog with someone you know who is facing or recovering from a neck dissection surgery. Let’s help them get the support they need to recover.)